Pharmacotherapeutic group: drugs for dementia.
ATC-code: N06DA02.
Pharmacology: Pharmacodynamics: Donepezil hydrochloride is a specific and reversible inhibitor of acetylcholinesterase, the predominant cholinesterase in the brain. Donepezil hydrochloride is
in vitro over 1000 times more potent an inhibitor of this enzyme than of butyrylcholinesterase, an enzyme which is present mainly outside the central nervous system.
Clinical trials: Mild to Moderately Severe Alzheimer's disease: In patients with Alzheimer's dementia participating in clinical trials, administration of single daily doses of 5 mg or 10 mg of ARICEPT produced steady-state inhibition of acetylcholinesterase activity (measured in erythrocyte membranes) of 63.6% and 77.3%, respectively when measured post dose. The inhibition of acetylcholinesterase (AChE) in red blood cells by donepezil hydrochloride has been shown to correlate to changes in ADAS-cog, a sensitive scale which examines selected aspects of cognition. The potential for donepezil hydrochloride to alter the course of the underlying neuropathology has not been studied. Thus donepezil hydrochloride (ARICEPT) cannot be considered to have any effect on the progress of the disease.
Efficacy of treatment of Alzheimer's dementia with ARICEPT has been investigated in four placebo-controlled trials, 2 trials of 6-month duration and 2 trials of 1-year duration. In the 6-month clinical trial, an analysis was done at the conclusion of donepezil hydrochloride treatment using a combination of three efficacy criteria: the ADAS-cog (a measure of cognitive performance), the Clinician Interview Based Impression of Change with Caregiver Input (a measure of global function) and the Activities of Daily Living Subscale of the Clinical Dementia Rating Scale (a measure of capabilities in community affairs, home and hobbies and personal care). Patients who fulfilled the criteria listed as follows were considered treatment responders.
Response = Improvement of ADAS-cog of at least 4 points; No deterioration of CIBIC; No deterioration of Activities of Daily Living Subscale of the Clinical Dementia Rating Scale. (See Table 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
ARICEPT produced a dose-dependent statistically significant increase in the percentage of patients who were judged treatment responders.
Severe Alzheimer's Disease: Efficacy of treatment with ARICEPT 10mg in severe Alzheimer's disease has been investigated in three placebo-controlled trials of 6-month duration. In each of the clinical trials, an analysis was done at the conclusion of donepezil hydrochloride treatment using a combination of three efficacy criteria: the total Severe Impairment Battery (SIB - a measure of cognitive performance in all three trials) score, the Clinician's Interview Based Impression of Change with caregiver input (CIBIC+ - a measure of global function in two trials) or Clinical Global Impression of Change (CGI-I - a measure of global function in one trial) and the modified Alzheimer's Disease Cooperative Study - Activities of Daily Living inventory for severe Alzheimer's disease (ADCS-ADL-sev - a measure of function in all three trials).
Patients who fulfilled the criteria listed as follows were considered treatment responders.
Response = Improvement of SIB of at least 4 points; No deterioration of CIBIC+ or CGI-I; No deterioration of ADCS-ADL-sev. (See Table 2.)
Click on icon to see table/diagram/image
The effectiveness of ARICEPT Film-coated Tablets 23 mg as a treatment for moderate to severe Alzheimer's disease compared to donepezil hydrochloride 10 mg has been demonstrated by the results of a randomized, double-blind, controlled clinical investigation in patients with moderate to severe Alzheimer's disease. The controlled clinical study was conducted globally in patients with probable Alzheimer's disease diagnosed by NINCDS-ADRDA and DSM-IV criteria, MMSE: range of 0-20. Patients were required to have been on a stable dose of ARICEPT 10 mg/day for at least 3 months prior to screening.
One thousand four hundred and thirty four (1434) patients with moderate to severe Alzheimer's disease were randomized to 23 mg/day or 10 mg/day. The mean age of patients was 73.8 years, with a range of 47 to 90. Approximately 63% of patients were women, and 37% were men. Approximately 36% of the patients were taking memantine throughout the study.
Study Outcome Measures: The effectiveness of treatment with ARICEPT Film-coated Tablets 23 mg was determined using a dual outcome assessment strategy that evaluated cognitive function using an instrument designed for more impaired patients and overall function through caregiver-rated assessment. This study showed that patients on ARICEPT Film-coated Tablets 23 mg experienced important clinical benefit on both measures compared to donepezil hydrochloride 10 mg/day. The ability of ARICEPT Film-coated Tablets 23 mg to improve cognitive performance was assessed with the Severe Impairment Battery (SIB). The SIB, a multi-item instrument, has been validated for the evaluation of cognitive function in patients with moderate to severe dementia. The SIB evaluates selective aspects of cognitive performance, including elements of memory, language, orientation, attention, praxis, visuospatial ability, construction, and social interaction. The SIB scoring range is from 0 to 100, with lower scores indicating greater cognitive impairment.
The ability of ARICEPT Film-coated Tablets 23 mg to produce an overall clinical effect was assessed using a Clinician's Interview-Based Impression of Change that incorporated the use of caregiver information, the CIBIC-plus. The CIBIC-plus used in this trial was a semi-structured instrument that examines four major areas of patient function: General, Cognitive, Behavioral and Activities of Daily Living. It represents the assessment of a skilled clinician based upon his/her observations at an interview with the patient, in combination with information supplied by a caregiver familiar with the behavior of the patient over the interval rated. The CIBIC-plus is scored as a seven point categorical rating, ranging from a score of 1, indicating "markedly improved" to a score of 4, indicating "no change" to a score of 7, indicating "markedly worse".
Effects on the SIB: Figure 1 shows the time course for the change from baseline in SIB score for the two treatment groups over the 24 weeks of the study. At 24 weeks of treatment, the LS mean difference in the SIB change scores for ARICEPT Film-coated Tablets 23 mg treated patients compared to patients treated with 10 mg donepezil hydrochloride was 2.2 units (p <0.0001). ARICEPT Film-coated Tablets 23 mg was statistically significantly superior to 10 mg donepezil hydrochloride. (See Figure 1.)
Click on icon to see table/diagram/image
Figure 2 illustrates the cumulative percentages of patients from each of the two treatment groups who attained the measure of improvement in SIB score shown on the X-axis. While patients assigned both to ARICEPT Film-coated Tablets 23 mg and to donepezil hydrochloride 10 mg tablets have a wide range of responses, the curves show that the ARICEPT Film-coated Tablets 23 mg group is more likely to show a greater improvement in cognitive performance. When such curves are shifted to the left, this indicates a greater percentage of patients responding to treatment on the SIB. (See Figure 2.)
Click on icon to see table/diagram/image
Effects on the CIBIC-plus: Figure 3 is a histogram of the frequency distribution of CIBIC-plus scores attained by patients at the end of 24 weeks of treatment. The mean difference between ARICEPT Film-coated Tablets 23 mg and donepezil hydrochloride 10 mg tablets was 0.06 units. The difference was not statistically significant. (See Figure 3.)
Click on icon to see table/diagram/image
Pharmacokinetics: General characteristics: Absorption: Maximum plasma levels are reached approximately 3 to 4 hours after oral administration for ARICEPT EVESS 5mg and 10mg orodispersible tablets. Based on population pharmacokinetic analysis of plasma donepezil hydrochloride concentrations measured in patients with Alzheimer's disease, following oral dosing, peak plasma concentration is achieved for ARICEPT Film-coated Tablets 23 mg in approximately 8 hours. Peak plasma concentrations were almost 2-fold higher for ARICEPT Film-coated Tablets 23 mg than ARICEPT 10 mg tablets. The elimination half life of donepezil hydrochloride is about 70 hours and the mean apparent plasma clearance (Cl/F) is 0.13 - 0.19 L/hr/kg. Following multiple dose administration, donepezil hydrochloride accumulates in plasma by 4-7 fold, and steady state is reached within 15 days. Once at steady-state, plasma donepezil hydrochloride concentrations and the related pharmacodynamic activity show little variability over the course of the day. Food did not affect the absorption of donepezil hydrochloride.
Distribution: The steady state volume of distribution is 12-16 L/kg. Donepezil hydrochloride is approximately 96% bound to human plasma proteins, mainly to albumins (about 75%) and alpha-1-acid glycoprotein (about 21%) over the concentration range of 2-1000 ng/mL. The plasma protein binding of the active metabolite 6-O-desmethyl donepezil is not known. The distribution of donepezil hydrochloride in various body tissues has not been definitively studied. However, in a mass balance study conducted in healthy male volunteers, 240 hours after the administration of a single 5 mg dose of
14C-labeled donepezil hydrochloride, approximately 28% of the label remained unrecovered. This suggests that donepezil hydrochloride and/or its metabolites may persist in the body for more than 10 days.
Metabolism/Excretion: Donepezil hydrochloride is both excreted in the urine intact and extensively metabolized to four major metabolites, two of which are known to be active, and a number of minor metabolites, not all of which have been identified. Donepezil hydrochloride is metabolized by CYP 450 isoenzymes 2D6 and 3A4 and undergoes glucuronidation. Following administration of
14C-labeled donepezil hydrochloride, plasma radioactivity, expressed as a percent of the administered dose, was present, primarily as intact, donepezil hydrochloride (53%) and as 6-O-desmethyl donepezil (11%), which has been reported to inhibit AChE to the same extent, as donepezil hydrochloride in vitro and was found in plasma at concentrations equal to about 20% of donepezil hydrochloride. Approximately 57% and 15% of the total radioactivity was recovered in urine and feces, respectively, over a period of 10 days, while 28% remained unrecovered, with about 17% of the donepezil hydrochloride dose recovered in the urine as unchanged drug. Examination of the effect of CYP2D6 genotype in Alzheimer's patients showed differences in clearance values among CYP2D6 genotype subgroups. When compared to the extensive metabolizers, poor metabolizers had a 31.5% slower clearance and ultra-rapid metabolizers had a 24% faster clearance. These results suggest CYP2D6 has a minor role in the metabolism of donepezil hydrochloride.
Hepatic Disease: In a study of 10 patients with stable alcoholic cirrhosis, the clearance of donepezil hydrochloride was decreased by 20% relative to 10 healthy age-matched and sex-matched subjects.
Renal Disease: In a study of 11 patients with moderate to severe renal impairment (Cl
c <18 mL/min/1.73 m
2) the clearance of donepezil hydrochloride did not differ from 11 age-matched and sex-matched healthy subjects.
Age: No formal pharmacokinetic study was conducted to examine age-related differences in the pharmacokinetics of ARICEPT. Population pharmacokinetic analysis suggested that the clearance of donepezil hydrochloride in patients decreases with increasing age. When compared with 65-year old subjects, 90-year old subjects have a 17% decrease in clearance, while 40-year old subjects have a 33% increase in clearance. The effect of age on donepezil hydrochloride clearance may not be clinically significant.
Gender and Race: No specific pharmacokinetic study was conducted to investigate the effects of gender and race on the disposition of ARICEPT. However, retrospective pharmacokinetic analysis and population pharmacokinetic analysis of plasma donepezil hydrochloride concentrations measured in patients with Alzheimer's disease indicates that gender and race (Japanese and Caucasians) did not affect the clearance of ARICEPT to an important degree.
Body weight: There was a relationship noted between body weight, and clearance. Over the range of weights from 50 kg to 110 kg, clearance increased from 7.77 L/h to 14.04 L/h, with a value of 10 L/h for 70 kg individuals.
Drugs Highly Bound to Plasma Proteins: Drug displacement studies have been performed in vitro between this highly bound drug (96%) and other drugs such as furosemide, digoxin, and warfarin. Donepezil hydrochloride at concentrations of 0.3-10 μg/mL did not affect the binding of furosemide (5 μg/mL), digoxin (2 ng/mL), and warfarin (3 μg/mL) to human albumin. Similarly, the binding of donepezil hydrochloride to human albumin was not affected by furosemide, digoxin and warfarin.
Toxicology: Preclinical safety data: Extensive testing in experimental animals has demonstrated that this compound causes few effects other than the intended pharmacological effects consistent with its action as a cholinergic stimulator (see Overdosage). Donepezil hydrochloride is not mutagenic in bacterial and mammalian cell mutation assays. Some clastogenic effects were observed
in vitro at concentrations overtly toxic to the cells and more than 3000 times the steady-state plasma concentrations. No clastogenic or other genotoxic effects were observed in the mouse micronucleus model
in vivo.
There was no evidence of oncogenic potential in long term carcinogenicity studies in either rats or mice. No evidence of a carcinogenic potential was obtained in an 88-week carcinogenicity study of donepezil hydrochloride conducted in CD-1 mice at doses up to 180 mg/kg/day (approximately 40 times the maximum recommended human dose of 23 mg/day on a mg/m
2 basis), or in a 104-week carcinogenicity study in Sprague-Dawley rats at doses up to 30 mg/kg/day (approximately 13 times the maximum recommended human dose on a mg/m
2 basis). Donepezil hydrochloride had no effect on fertility in rats and was not teratogenic in rats or rabbits, but had a slight effect on stillbirths and early pup survival when administered to pregnant rats at 50 times the human dose (see Use in Pregnancy & Lactation).




 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image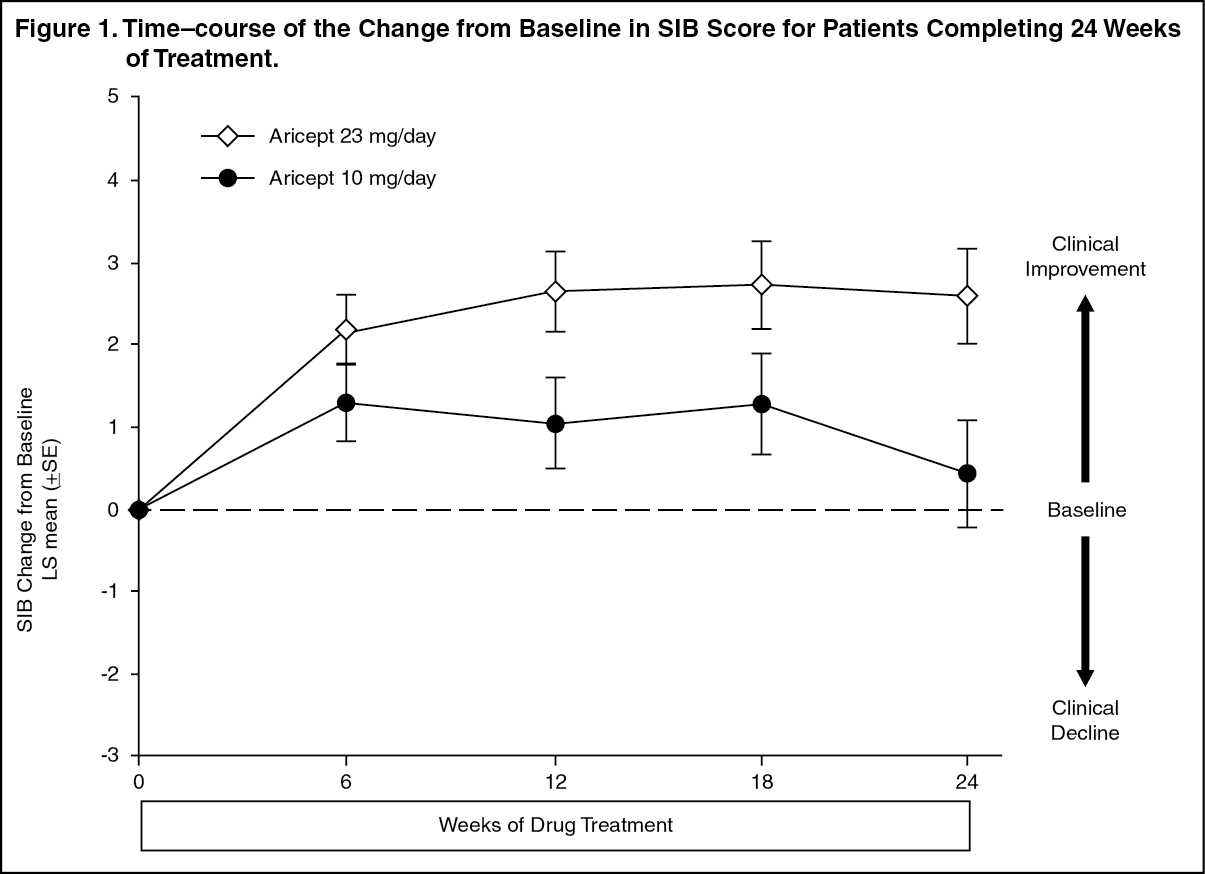 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image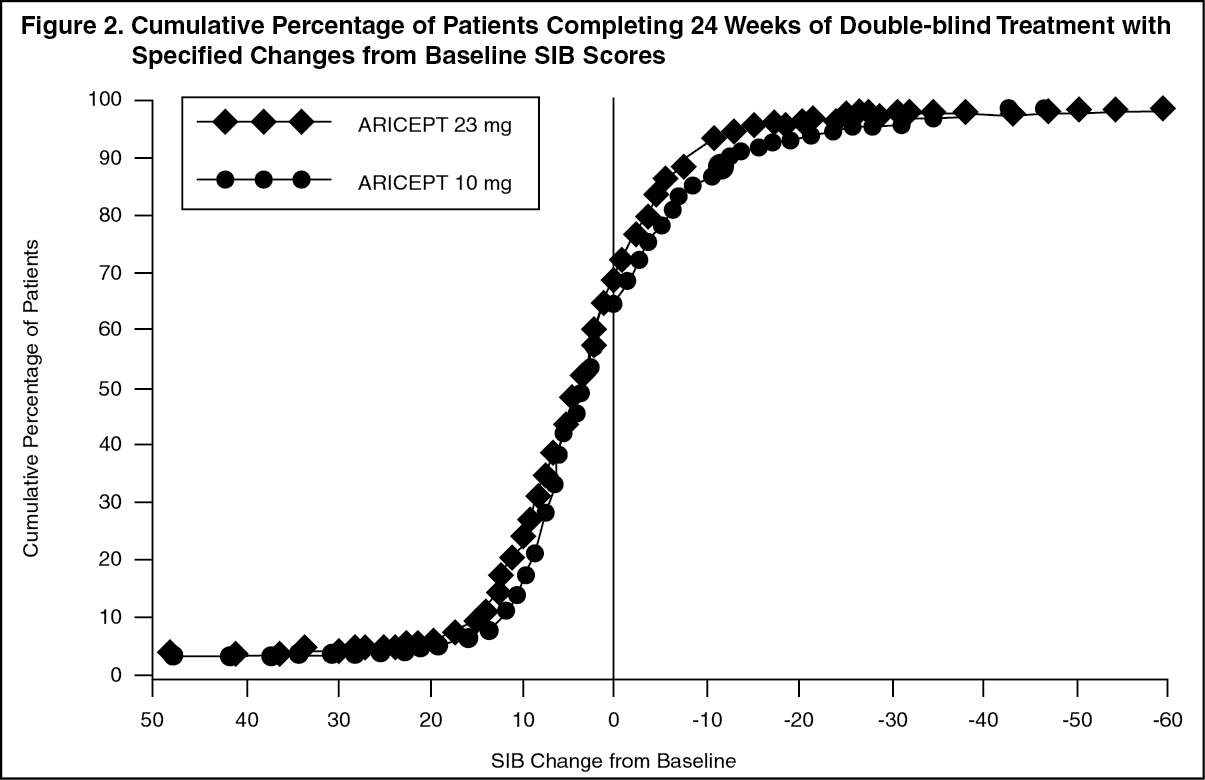 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image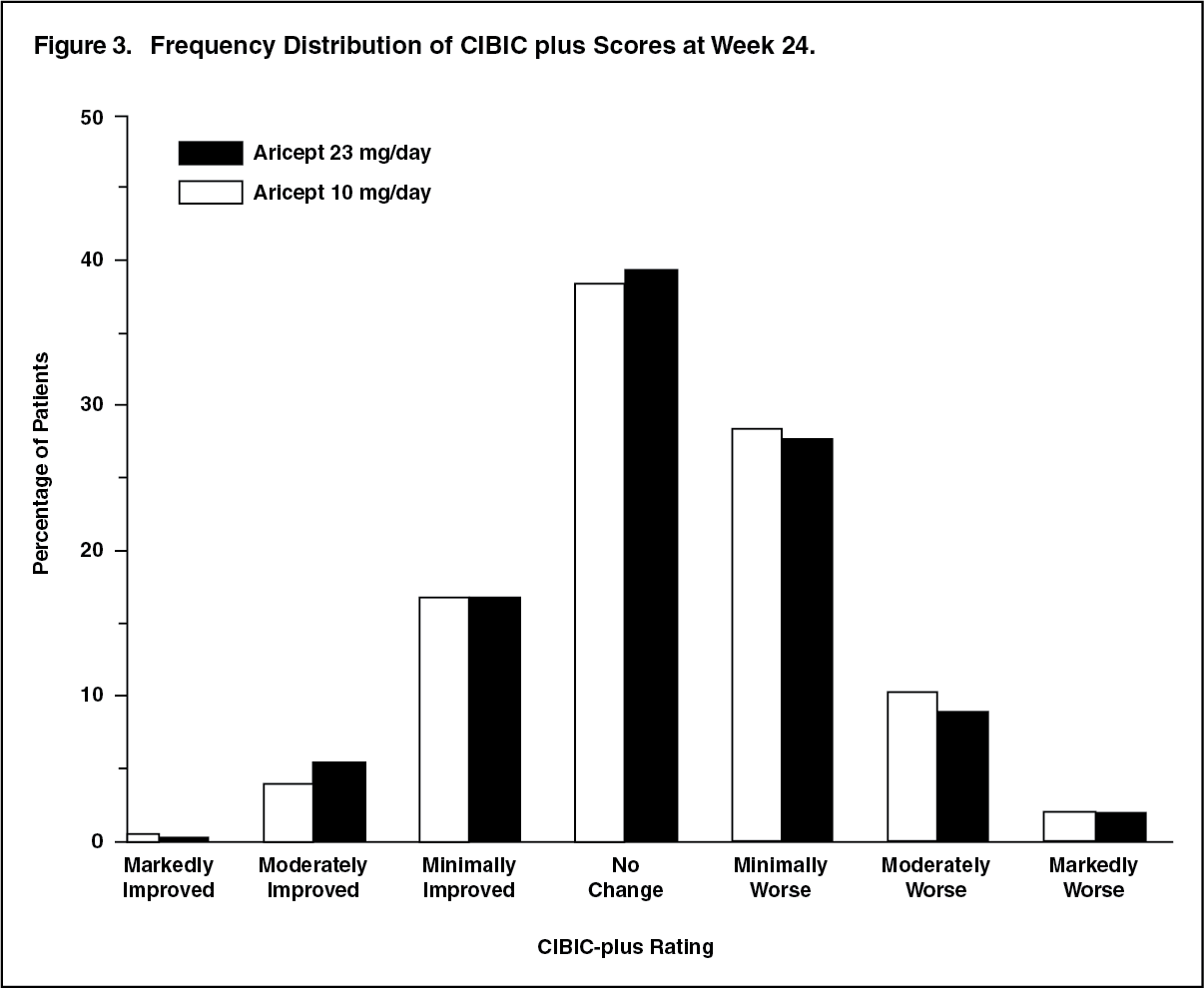 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image



 Sign Out
Sign Out